
Ebola is a rare but severe viral illness that causes outbreaks of hemorrhagic fever, primarily in sub-Saharan Africa. With fatality rates ranging from 25% to 90% depending on the strain, Ebola has been a significant public health concern since it was first identified in 1976 in what is now the Democratic Republic of the Congo. In May 2026, the World Health Organization declared a Public Health Emergency of International Concern as a new outbreak of the Bundibugyo strain spread across eastern DRC and into neighboring Uganda.
What Causes Ebola? Understanding the Virus Behind the Disease
Ebola disease is caused by infection with orthoebolaviruses, a group of filoviruses found primarily in sub-Saharan Africa. These viruses were first discovered in 1976 near the Ebola River in the Democratic Republic of the Congo, which gave the disease its name. There are four types of orthoebolaviruses known to cause illness in humans: Ebola virus (Zaire ebolavirus), Sudan virus, Taï Forest virus, and Bundibugyo virus. Two additional types—Reston virus and Bombali virus—have not been known to cause disease in humans.
Each strain differs in its severity and geographic distribution. The Ebola virus (Zaire species) is the most common and deadly, responsible for the largest outbreaks including the 2014-2016 West Africa epidemic. The Bundibugyo virus, which is driving the 2026 outbreak, has historically caused death rates between 25% and 50%. Scientists believe African fruit bats serve as natural reservoirs for orthoebolaviruses, with primates and other mammals also susceptible to infection.
How Ebola Spreads: Transmission Routes Explained
Ebola is not airborne and cannot be transmitted through coughing or sneezing. The virus spreads exclusively through direct contact with body fluids of infected individuals or contaminated objects. Understanding this transmission pathway is crucial for effective prevention.
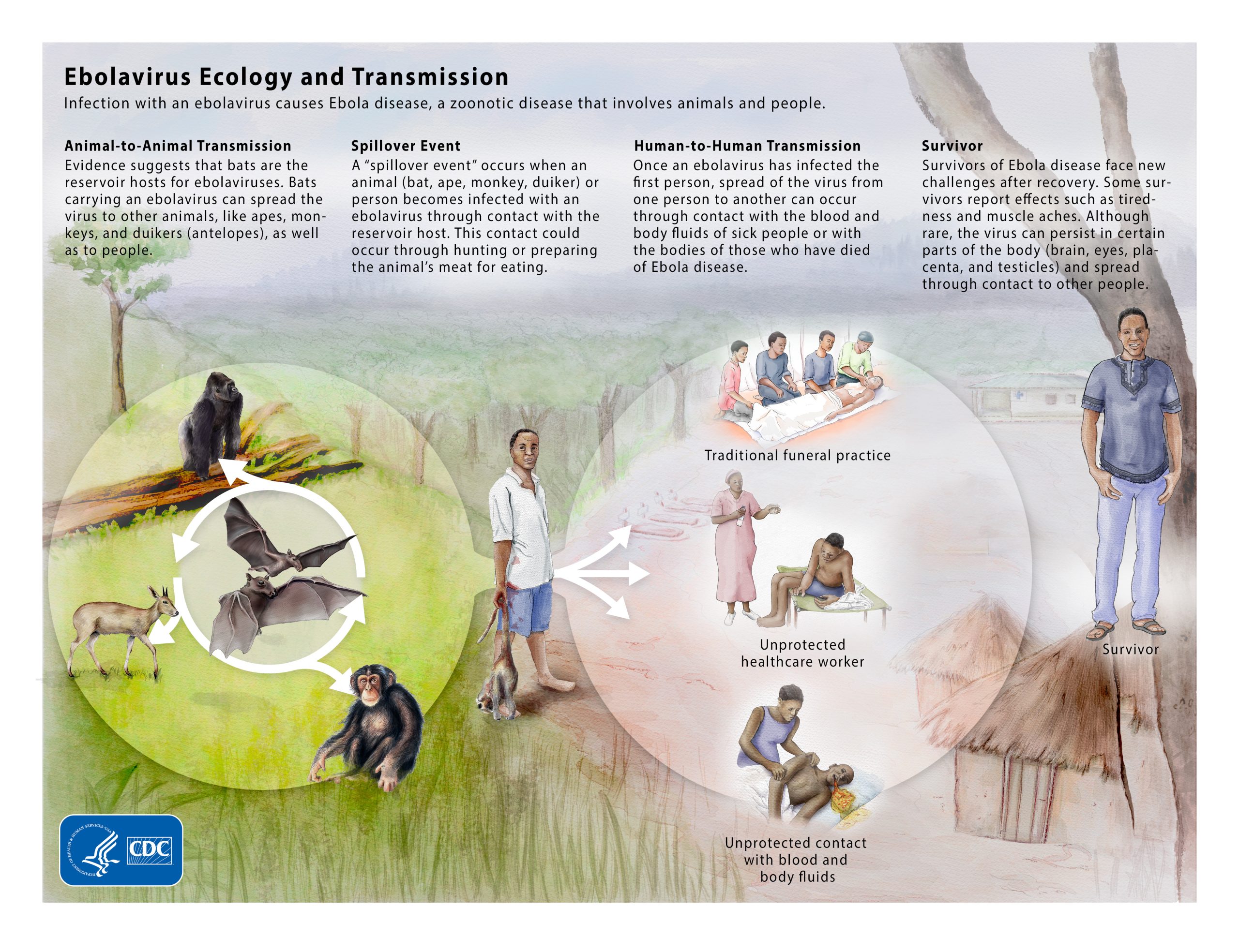
From animals to humans: The initial infection in a human population, called a spillover event, typically occurs when someone comes into contact with the blood, secretions, organs, or other body fluids of infected animals. This can happen through hunting, handling, or eating infected bats, forest antelopes, or non-human primates.
Human-to-human transmission: Once a spillover occurs, the virus spreads between people when broken skin or mucous membranes in the eyes, nose, or mouth come into contact with blood, urine, saliva, sweat, feces, vomit, breast milk, amniotic fluid, or semen from an infected person. Contaminated objects like clothing, bedding, needles, and medical equipment can also transmit the virus. People become infectious only after they develop symptoms, typically 8 to 10 days after exposure.
Transmission after recovery: Advances in treatment mean more people are surviving Ebola. However, the virus can remain in certain body parts shielded from the immune system, particularly in the semen of male survivors. Sexual transmission can occur even months after recovery, which is why ongoing monitoring is essential.
Signs and Symptoms: From First Signs to Severe Illness
Ebola symptoms appear 2 to 21 days after exposure, with the average incubation period being 8 to 10 days. The illness progresses through distinct phases that healthcare providers categorize as "dry" and "wet" symptoms.
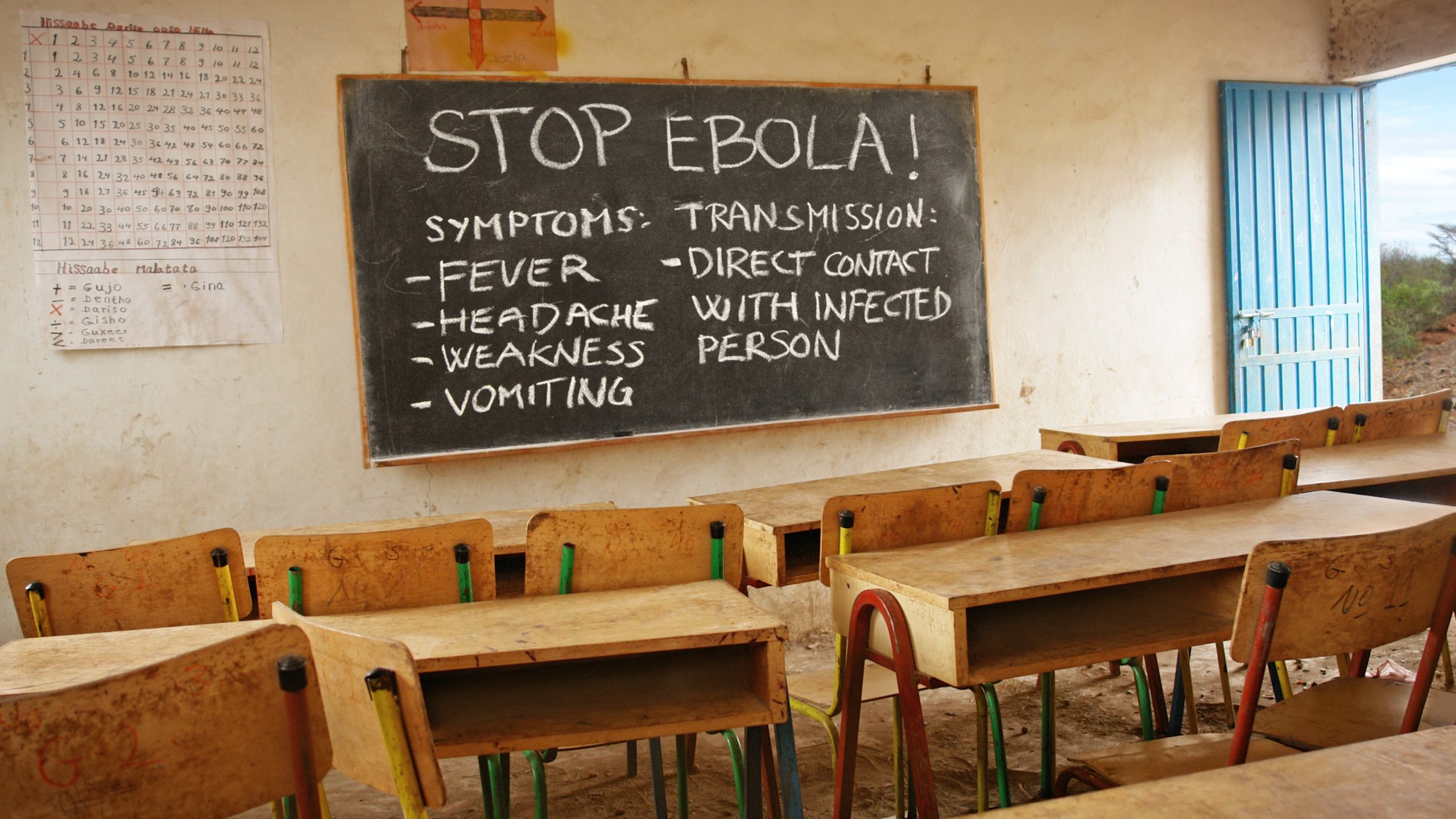
Early "dry" symptoms include fever, severe headache, muscle and joint pain, weakness and fatigue, sore throat, and loss of appetite. These flu-like symptoms are nonspecific, making early diagnosis challenging. Healthcare providers may initially confuse Ebola with malaria, influenza, typhoid fever, or other common infectious diseases.
Progression to "wet" symptoms typically occurs within a few days and includes vomiting (which may be bloody), diarrhea, abdominal pain, rash, red or bloodshot eyes, and unexplained bleeding or bruising. As the disease advances, patients may develop more severe complications including impaired kidney and liver function, organ failure, and encephalitis (brain inflammation). The severe bleeding that gives Ebola its reputation as a hemorrhagic fever occurs in later stages.
Diagnosis and Treatment: How Ebola Is Managed
Diagnosing Ebola requires laboratory testing, primarily through polymerase chain reaction (PCR) blood tests that detect the virus's genetic material. Antibody testing can also determine if someone has recently been infected. Patients being tested should be isolated from others until results are confirmed to prevent potential spread.
Available treatments: The U.S. Food and Drug Administration has approved two treatments specifically for Ebola virus (Zaire species): Inmazeb (a combination of three monoclonal antibodies) and Ebanga (a single monoclonal antibody). These treatments significantly improve survival rates when administered early. For other strains like the Bundibugyo virus currently circulating in the 2026 outbreak, no specific antiviral treatments are approved, and care focuses on supportive measures.
Supportive care is critical regardless of the strain. Patients have a much better chance of survival when they receive fluids and electrolytes (by mouth or intravenously), medications to support blood pressure and manage symptoms like vomiting and diarrhea, pain management, and treatment for any secondary infections. The supportive care approach has dramatically improved survival rates compared to earlier outbreaks.
Prevention: How to Protect Against Ebola
Prevention centers on avoiding contact with the virus and, where available, using vaccination. The CDC recommends several key measures for people in or traveling to affected regions.
Vaccination: The FDA has approved ERVEBO (rVSV-ZEBOV) for the prevention of Ebola disease caused by the Zaire species. This vaccine is recommended for adults 18 years and older who are at potential risk of exposure, including healthcare workers and laboratory personnel. Critically, no approved vaccine currently exists for the Bundibugyo virus, which is the strain responsible for the 2026 outbreak in DRC and Uganda.
Infection control measures include avoiding direct contact with blood and body fluids of infected individuals, using proper personal protective equipment (PPE) when caring for patients, practicing safe burial practices that respect cultural traditions while minimizing exposure risk, and avoiding contact with bats, primates, and raw meat from these animals in affected areas. Travelers returning from regions with ongoing outbreaks should monitor their health for 21 days and seek immediate medical care if symptoms develop.

The 2026 Bundibugyo Outbreak: Current Situation
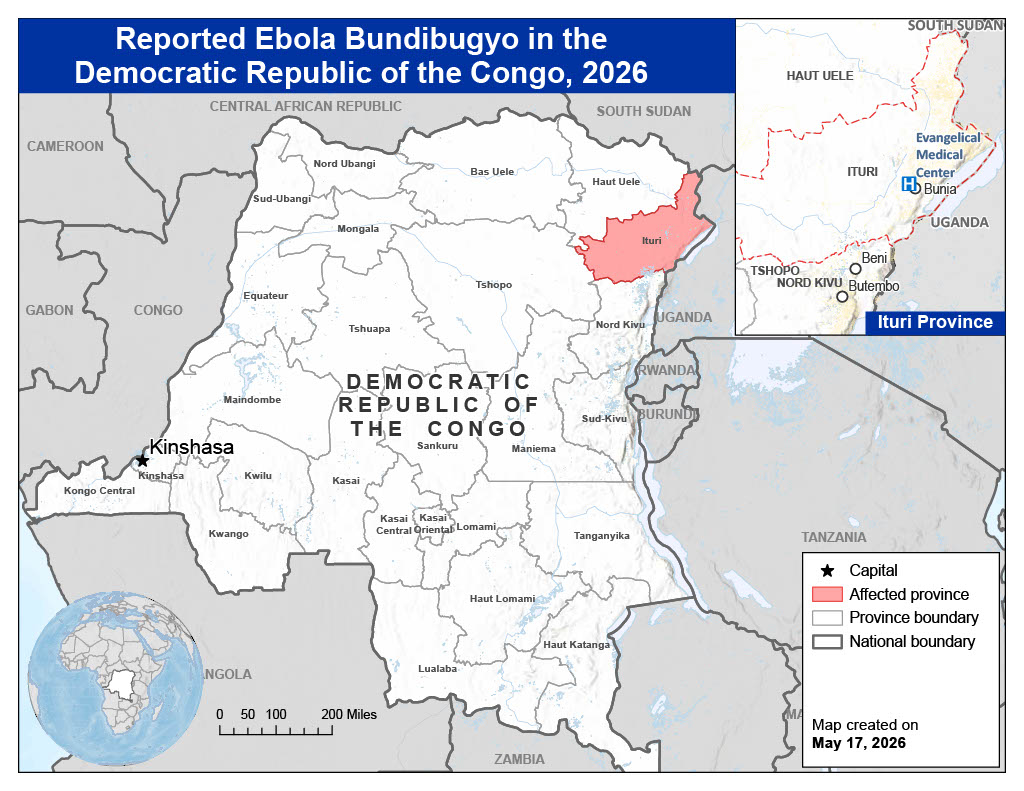
As of May 19, 2026, a fast-spreading Ebola outbreak caused by the Bundibugyo virus is unfolding in the Democratic Republic of the Congo and Uganda. The outbreak was first detected in early May when a hospital in Bunia Health Zone in northeastern DRC identified a cluster of severe illnesses affecting healthcare workers. On May 15, genetic fingerprinting confirmed the pathogen as Bundibugyo virus, and on May 17, the WHO declared the situation a Public Health Emergency of International Concern.
Key numbers from the outbreak:
- 536 suspected cases, 105 probable cases, and 34 confirmed cases reported
- At least 134 deaths, including 80 suspected deaths in Ituri Province
- The outbreak has spread to 9 health zones in Ituri Province
- Two confirmed cases and one death reported in Uganda among people who traveled from DRC
- An American healthcare worker who was exposed while caring for patients in DRC tested positive and was transported to Germany for treatment
On May 18, the CDC and the U.S. Department of Homeland Security implemented enhanced travel screening and entry restrictions to prevent Ebola from entering the United States. These measures include screening travelers arriving from DRC, Uganda, and South Sudan, and restricting entry for non-U.S. passport holders who have been in these countries within the previous 21 days. To date, no cases related to this outbreak have been confirmed in the United States.
The WHO is considering the use of experimental vaccines for the Bundibugyo strain, but no vaccine is currently available, and any potential rollout remains months away. WHO's representative in DRC, Dr. Anne Ancia, reported that more than 500 suspected cases have been identified, with testing kits being rushed to eastern DRC to accelerate case identification.
Key Takeaways: What You Need to Know About Ebola
- Ebola is caused by a virus, not spread through air or water, requiring direct contact with body fluids for transmission
- Symptoms appear 2-21 days after exposure, beginning with fever and fatigue and potentially progressing to severe vomiting, diarrhea, and bleeding
- Treatment is available for the Zaire strain (two FDA-approved drugs), but the 2026 outbreak involves Bundibugyo, for which only supportive care exists
- A vaccine exists only for the Zaire strain (ERVEBO); no vaccine is currently approved for the Bundibugyo virus
- The overall risk to the general public and travelers remains low, with enhanced screening measures in place at U.S. ports of entry
- Early supportive care dramatically improves survival, making prompt medical attention critical if exposure is suspected
